


Cycle Myths or Truths? 👀
Damaging myths I STILL here confusion about among my girlfriends and clients.

Lily is a certified FAM teacher, herbalist and public health professional. The big idea behind this Substack is we deserve to know ALL the options when it comes to our reproductive health choices. Here we aim to fill in the gaps.
OK…what do you think?
1. Hormonal contraception regulates the menstrual cycle.
—True or false? Why?
2. Menstruation or bleeding is the main ‘event’ of the cycle.
—True or false? Why?
3. There is always some risk of pregnancy.
—True or false? Why?
Let’s unpack them one by one.
Hormonal contraception regulates the menstrual cycle.
Short answer: Absolutely not! It shuts down and replaces the hormones (estrogen and progesterone) normally produced through our ovaries. The synthetic hormones stop the natural processes—there IS no naturally occurring cycle to regulate, only a monotonous hormonal interference, broken by withdrawal bleeding (if on most common forms of hormonal contraception).
If you go this one wrong, it’s very understandable. This myth is at the heart of modern hormonal contraception. Contraception has been used as the panacea for a wide range of ailments—reproductive and otherwise— including dysmenorrhea (severe period pain), irregular cycles, acne and more.
If hormonal contraception regulated the menstrual cycle, it would mean it brought about more balance or uniformity. Imagine a cycle with erratic lengths becoming predictable.
While most forms of hormonal contraception appear to regulate (the why behind that worthy of a separate post) they are in fact stopping ovulation and the cascade of hormones that lead up to it (hormonal IUDs can sometimes be an exception). Ovulation (not bleeding) is the key event of a menstrual cycle. It’s a prerequisite for naturally occurring conception.
Regulate: to bring order, method, or uniformity to
Stop: to close by filling or obstructing or to hinder or prevent the passage of
For this simple reason, hormonal birth control is not regulating, it’s stopping the normal process in its tracks.
Getting nerdy with me—more deets:
To understand this, take a moment to consider our cycle our cycle as a perfectly orchestrated cascade of events.
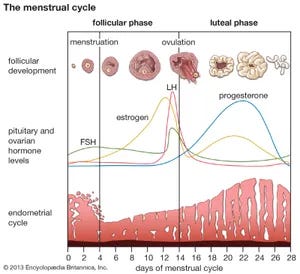
Cyclical changes during a woman's normal ovulatory menstrual cycle. Encyclopædia Britannica, Inc.
Each, executed successfully triggers the next. Low estrogen triggers release of Follicle Stimulating Hormone (FSH), which speeds the growth of already maturing follicles (containing eggs), as the follicles mature they release more estrogen, which eventually triggers Luteinizing Hormone. LH triggers ovulation—the egg that has grown dominant is released. It’s follicle, left behind, transforms into the corpus luteum or yellow body. The corpus luteum releases progesterone, which thickens our cervical mucus, and prepares the endometrium for possible implantation. The thick mucus serves as a protective barrier; sperm and other foreign agents are no longer welcome.
If fertilization and implantation do not occur—aka we aren’t pregnant, the corpus luteum breaks downs and progesterone levels drop, triggering the shedding of our our endometrium. From there it starts over; beginning with the negative feedback loop of low estrogen which triggers a pituitary hormone (GnRH) to produce FSH and so on and so forth through our productive years.
Hormonal contraception works by interfering with this cascade. Constant low levels of synthetic estrogen mean our bodies own estrogen is suppressed, and thus the maturation of follicles and eggs is stymied. Progestin—likewise acts to stop any potential sperm through creating inhospitable cervical mucus—the kind we usually have AFTER we ovulate.
Ovulation is the main event of the menstrual cycle. Bleeding is a byproduct.
OK—now that you understand the above, this one is likely pretty clear.
Everything the body does in a menstrual—or can we just say ovulation —cycle —centers around ovulation. Ovulation is queen. She’s the PURPOSE of the cycle. She’s a sign of health. If our body is in survival mode—we’re not eating enough, we’re overly stressed, we’re sick, etc we may not ovulate at all (research has found it’s normal for women with cycles that are within normal health parameters to have 1-2 anovulatory cycles per year).
As described above, bleeding is a result of a cycle that ended without fertilization and implantation.
To have a period, we have to ovulate, thus, the bleed experienced when taking hormonal contraception is not menstruation. It is withdrawal bleeding. The interruption in synthetic hormones leads to a shedding of the uterine lining. The blood will typically be thinner and less developed than what is expected during an ovulation cycle, where our natural hormones led the development of a thick lining suitable to nurture new life.
Pregnancy can only occur during a limited window surrounding ovulation.
If you grew up in the 90s and early 2000s like me, you may have been tricked into believing you could become pregnant at any moment. I’ll never forgot the two times a condom slipped and I dashed to the pharmacy to swallow down Plan B. After the second time, I found myself a gyno and got an IUD I wore for years.

But here’s the truth:
We have a limited fertile window. If I had been using a sympto-thermal tracking method, I would have at least know IF it was even possible for me to get pregnant, saving cash and definitely stress.
Our fertile window is influenced by two factors:
a- egg life; once we ovulate—one of our ovaries releases an egg—the egg will live up to 24 hours. Once the egg disintegrates, we can no longer get pregnant during that cycle. (In rare cases, an ovary releases a second egg within 24 hours of the first, this possibility is accounted for if you use a cycle tracking method for contraception).
b-sperm life; our bodies are crafty. Depending on our cervical mucus, sperm can expire in minutes or live up to 5 days. The rise in estrogen (see above) causes an increase in fertile mucus that is nourishing to sperm. Thus, there is the potential to have sex up to 5 days prior to ovulation and get pregnant. Our true fertile window is thus ~ 6 days.
Most fertility awareness methods (FAM), instruct to consider any days with estrogenic mucus fertile since we cannot predict the exact day of ovulation until it happens. We also consider the three days after ovulation as fertile *when trying to prevent pregnancy—*a precaution based on the rare second egg scenario.
So where does that leave us? There are 2-3 weeks of every cycle where there is no chance you can get pregnant.
So how’d you do? 3/3, 2/3, less? What do YOU think are the most damaging myths around the ovulation cycle?
Herbalist and ovulation cycle coach, Lily Sussman, works to set the women free from big pharma, offering a chance for much better health. Artificial birth control has been a mess from day 1, and has caused women to need additional healthcare and meds. There are effective natural methods ready for the skillful operator who is wishes to take charge of her health.